Nghiên cứu về các tác động của việc chuyển giao đối với chương trình MMT
Bạn đang xem bản rút gọn của tài liệu. Xem và tải ngay bản đầy đủ của tài liệu tại đây (1.96 MB, 8 trang )
<span class='text_page_counter'>(1)</span><div class='page_container' data-page=1>
<b>EFFECTS OF THE TRANSITION </b>
<b>FROM A FREE-SERVICE MODEL </b>
<b>TO A CO-PAY MODEL IN THE </b>
<b>METHADONE MAINTENANCE </b>
<b>TREATMENT PROGRAM</b>
USAID SMART TA Technical Report
Hai Phong, Vietnam, 2013-2014
<b>RESEARCH TEAM</b>
Nguyen To Nhu, MD, PhD
<b>Principal Investigator</b>
</div>
<span class='text_page_counter'>(2)</span><div class='page_container' data-page=2></div>
<span class='text_page_counter'>(3)</span><div class='page_container' data-page=3>
<b>CONTEXT </b>
The National Methadone Maintenance Treatment (MMT) program,
offering voluntary outpatient opioid replacement therapy, was launched
in Vietnam in 2008. After years of successful program outcomes, and in
light of reducing international funding to Vietnam, the Government of
Vietnam has taken steps to ensure the program’s long-term financial
sustainability. This includes shifting from a free-service model to
a co-pay mechanism, in which local governments and patients are
responsible for a major share of the operational costs. In Hai Phong
specifically, the People’s Committee issued Decision 2574/QD-UBND
instituting a temporary 10,000 VND (0.49 USD) fee per day, which took
effect on January 1, 2014 with an 80 percent subsidy for disadvantaged
or impoverished patients.
In response to concerns that the new fee
policy would cause patients to drop out
of the program, use opioids concurrently
or feel dissatisfied with the service, a
qualitative and quantitative study was
conducted in nine MMT clinics.
<b>METHODOLOGY</b>
This study utilized a mixed-method design
combining time-trend analysis, serial
cross-sectional surveys, focus group
discussions and in-depth interviews. Five
rounds of surveys were sent to MMT
patients with an 82 percent participation
rate (sample size = 2,102). Focus group
discussions were held with clinic staff and
in-depth interviews were carried out with
MMT patients who had dropped out of the
program voluntarily.
</div>
<span class='text_page_counter'>(4)</span><div class='page_container' data-page=4>
<b>FINDINGS</b>
<b>DROPOUT AND MISSED DOSES </b>
Although there was a statistically significant change in the average monthly
dropout rate between 2013 and 2014, it was only a 0.3 percent increase
and cannot be attributed solely to the payment installation in light of the
limited scope of this survey.<b> There was only a two percent drop in the </b>
<b>number of patients across all nine clinics in 2014, so any effect the </b>
<b>co-pay model had on dropout rates was marginal, if at all. </b>
<b>“The number of patients who quit for financial </b>
<b>reasons that we were aware of was just 3-4 </b>
<b>cases. Before stopping treatment, they hadn’t </b>
<b>paid for several months, then quit. It was not </b>
<b>that we refused to serve them, but that they </b>
<b>felt embarrassed until they decided to quit.” </b>
<b>(Counselor, Q1)</b>
There was also a small effect on the
number of missed doses. Patients
would skip doses on the days when
they were not able to pay, though
denying treatment was not part of
the new model.
<b>“According to our report, dose skipping is more </b>
<b>and more common.” </b>
<b>(Counselor, Q5) </b>
<b>“We don’t turn patients away, but they are self-aware and if they don’t have the </b>
<b>money, they don’t come.”</b>
<b> (Nurse, H4)</b>
</div>
<span class='text_page_counter'>(5)</span><div class='page_container' data-page=5>
<b>PATIENT SATISFACTION </b>
To evaluate any changes in patient satisfaction after
the institution of fee collection, a survey was sent out
every three months throughout the trial year for a
total of five surveys. Based on the results from the 82
percent participation rate from the 2,012 MMT patients,
<b>service satisfaction did initially drop after the co-pay </b>
<b>was rolled out but evened out over the course of the </b>
<b>survey collection.</b>
Other changes were seen in patient attitudes towards
MMT staff, with increased agitation, aggressiveness
and theft.
<b>“There have been some issues. Attitudes </b>
<b>of patients towards clinic staff have </b>
<b>changed. Previously, all clinic services </b>
<b>were free and there was no problem </b>
<b>with the relationship [between patients </b>
<b>and staff]. Now that a treatment fee is </b>
<b>collected, we have to remind patients </b>
<b>often. Regular reminders annoy patients, </b>
<b>and once they’re annoyed they heap </b>
<b>insults on us.”</b>
<b>(Nurse, Q2)</b>
<b>“When we tried to stop treatment for </b>
<b>some patients because they did not </b>
<b>pay their treatment fee, some became </b>
<b>aggressive and threatened us.” </b>
<b>(Receptionist, H3) </b>
<b>Clinic</b> <b>Average participation rate <sub>for 5 surveys (n=2,102)</sub></b>
An Duong 77%
An Hung 91%
An Lao 82%
Duong Kinh 84%
Hai An 87%
Hong Bang 80%
Le Chan 93%
Ngo Quyen 80%
Thuy Nguyen 67%
<b>TOTAL</b> <b>82%</b>
</div>
<span class='text_page_counter'>(6)</span><div class='page_container' data-page=6>
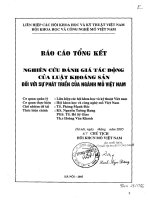
<b>FIGURE 1</b>
<b>Proportions of patients unsatisfied with services at nine MMT clinics in Hai Phong, </b>
<b>based on results of five serial surveys from February 2014 to February 2015.</b>
<b>Medical examination</b>
<b>Reception-administration</b>
<b>Counseling</b>
<b>Methadone dispensing</b>
<b>Security</b>
<b>Cleaning</b>
<b>Survey 1</b> <b>Survey 2</b> <b>Survey 3</b> <b>Survey 4</b> <b>Survey 5</b>
12
10
8
6
4
2
0
Despite some limitations and difficulties, providers held that the
collection of partial treatment costs helps improve staff incomes and
working conditions, which in turn help improve service quality.
<b>“For long-term operation of the MMT program, socialization is a must. If the patient </b>
<b>wants to be in long-term treatment, they must pay a portion of the treatment costs.” </b>
<b>(Head of clinic, H4)</b>
<b>WILLINGNESS TO PAY</b>
</div>
<span class='text_page_counter'>(7)</span><div class='page_container' data-page=7>
<b>ACKNOWLEDGMENTS</b>
<i>This research was made possible through support from USAID Vietnam under the project agreement # </i>
<i>AID-486-A-11-00011 “Sustainable Management of the HIV/AIDS Response and Transition to Technical Assistance” </i>
<i>(SMART TA) program. The research team included Dr. Nguyen Binh Nguyen, Dr. Pham Le Huy, Vuong Thi Anh Thu </i>
<i>and Nguyen Quynh Huong and was guided by Dr. Nguyen To Nhu. Special appreciation is also extended to the </i>
<i>Vietnam Administration of HIV/AIDS Control (VAAC), USAID team, PEPFAR MMT Technical Working Group in Vietnam, </i>
<i>Department of Harm Reduction VAAC, Hai Phong Provincial AIDS Center, Hai Phong Department of Health and the </i>
<i>nine methadone clinics and their patients that took part in this study. </i>
<i>This report was made possible by the generous support of the American people through the United States Agency for </i>
<i>International Development (USAID). The contents are the responsibility of FHI360 and do not necessarily reflect the </i>
<i>views of USAID or the United States Government.</i>
<b>For comments or questions, please contact:</b>
<b>Dr. Nguyen To Nhu, MD, PhD</b>
Deputy Country Director, FHI 360 Vietnam
<b>CONCLUSIONS</b>
There were small changes in the dropout and missed-dose rates among
MMT patients after the shift to a co-pay model, but there is not enough
evidence to determine if these were a direct result of the fee collection.
There were also changes in patient satisfaction, though the dissatisfaction
dissipated as people grew accustomed to the new system. Patients are
willing to pay for methadone overall, and instituting a fee for services
does not have major impacts on the MMT care system.
<b>RECOMMENDATIONS </b>
1. Set a regular monthly payment schedule, and explain the reasons
for the shift clearly to avoid surprises and misunderstandings when
collecting fees.
2. Hire an accountant to address the significant administrative burden
imposed on clinic staff during collection.
3. In light of the 30 percent of patients experiencing substantial or
extreme difficulty in paying for MMT, expand the categories eligible
for subsidies, or simplify the process required to request subsidies.
4. Clarify enforcement mechanisms or protocols in instances of
non-payment. Providers were unsure whether to deny treatment or
continue offering it, leading to confusion and unnecessary program
dropouts.
</div>
<span class='text_page_counter'>(8)</span><div class='page_container' data-page=8></div>
<!--links-->